 Loading...
Loading... Anatomy
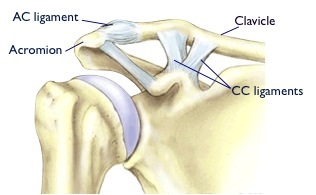
The acromioclavicular joint (ACJ) is situated on top of the shoulder joining the clavicle (the collar bone) to the acromion (the tip of the shoulder blade).
There are two ligaments which hold the collar bone in place. The acromioclavicular (AC) ligament attaches the clavicle to the scapula and prevents motion in the horizontal plane. The Coracoclavicular (CC) ligaments go from the coracoid process on the scapula to the clavicle and provide vertical stability.
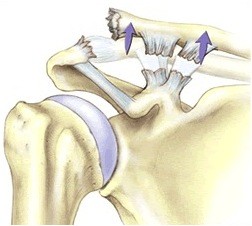
In a ACJ dislocation, one or both of the above ligaments are torn. Treatment is based on the severity of injury.
Mild cases where the step-off deformity is not severe can be treated in a sling. The sling is used for a few weeks and is followed by a course of physiotherapy. Surgery is usually reserved for cases with more severe displacement.
What does Surgery involve?
The surgery is a day-case and is performed arthroscopically (key hole).
Acute stabilisation is generally considered within 4 weeks from the injury and involves reduction and stabilisation of the Acromioclavicular Joint allowing the Coraco-Clavicular ligaments to heal restoring the stability of the joint.
Typically 2 small skin incisions are used, one at the side and one at the front of the shoulder. The undersurface of the coracoid is exposed and a special jig is used to enable a hole to be drilled through the clavicle and the coracoid.
The Tightrope system is then passed through the 2 holes and secured, reducing the Acromioclaviculat Joint in the correct position.
Following surgery the arm is placed in a sling for six weeks and the rehabilitation is supervised by a physiotherapist


 Arthroscopic
Arthroscopic